Access Denied? A new perspective on the cannula call
The anaesthetic team are responsible for providing routine and
emergency cover, both in and out of hours, in multiple areas
of the hospital. This includes but is not limited to, theatres,
intensive care units, emergency departments, maternity,
cardiac intervention, interventional radiology, airway support
for the base hospital, and on occasion, transfers between sites.
Vascular access is not a routine service that is provided by
most anaesthetic departments and is not feasible to add this
to the list of expected responsibilities of the anaesthetist. It is,
however, anecdotally noted to be the right thing to do, when
clinical workload allows, to assist a colleague from another
specialty.
The rationale often offered with regards to calling anaesthetics
is that should we be unable to secure venous access
peripherally, central access may be the logical next step.
Whilst we would agree with this in some circumstances, it adds
frustration to other specialties when we suggest that a senior
team member try in the first instance. As well as the most
senior member of the clinical team being placed to determine
whether the patient would be suitable for invasive access, they
also may be more experienced in gaining peripheral access in
less straightforward patients. This has benefits for patients by
reducing unnecessary, higher-risk procedures.
In these authors’ personal experience, these ‘tricky’ patients
referred to us often do not require any specialist equipment
and access can be successfully secured with patience and
doing basic techniques well. As pressure on the NHS and
with that, anaesthetic services, increases, it is likely that as a
specialty we will be unable to provide a sustainable vascular
access service, as indeed there often is not one.
Instead, these authors propose that anaesthetists could be
using these calls to our advantage to educate other medical
practitioners in effective techniques. This may help to reduce
demand and make the service accessible for those patients in
true need.
All avenues of medical practice require further learning.
If the anaesthetist is perceived as the most qualified to
perform difficult cannulation, then perhaps they are the
most appropriate to teach techniques for difficult peripheral
vascular access. This holds true in the authors’ opinion as most
“cannula calls” we have attended, have required nothing more
than a manual blood pressure cuff, an abundance of patience,
and in some circumstances, basic skills with an ultrasound
scanner. None of these things are specific to an anaesthetist
and are simple skills to develop if time is taken to teach and for
supervised practice.
Miller's Pyramid
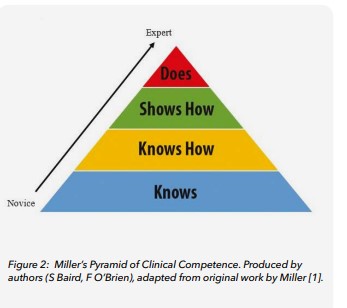
We propose a multi-step mastery education system, using
the top two layers of Miller’s pyramid of learning [1]; “shows
how” and “does” to ensure adequate learning. Miller’s Pyramid
is a framework developed to inform assessment of clinical
competency, utilising four steps as demonstrated in the
diagram below (Fig. 2).
Direct observation and feedback in simulation and finally in
practice are the final stages of this process “shows how” and
“does,” allowing assessment of technical and interpersonal
skills to prove competency. Examples of assessment at each
stage include MCQ assessments (factual recall) for “knows,”
case presentations for “knows how,” simulation and OSCEs
for “Shows how” and supervised learning events (e.g., direct
observation of procedural skills or DOPS) in the workplace,
all of which show progression from Novice to Expert.
How to improve peripheral vascular
access training
Firstly, an initial clinical teaching session, using cannulation
mannequins supervised by “expert” trainers (such as
anaesthetists), enabling supervised practice and critique of
technique. This may be best placed at Foundation Year 1 (FY1)
induction as these are the people most likely to be called first to
cannulate difficult patients.
Progression through this course of learning could potentially
take the form of supervised ultrasound scanning on live
volunteer models, which would allow participants to develop
an understanding of the relevant features on sonoanatomy e.g.,
ability to correctly identify arteries and veins from surrounding
tissue structures.
Finally, as part of this initial stage of learning, phantom needling
sessions could be arranged to allow for supervised practice and
ensure safety of needling technique.
However, all but the first step would be progression, and
focus should be on ensuring that the basics are done well one
hundred percent of the time. We also acknowledge that we are
privileged that most anaesthetic and intensive care, as well as
emergency departments, have an ultrasound scanner readily
available, whilst other areas do not have access to one at all.
This further validates the point that basic techniques and ways
to optimise difficult cases are the most important aspect.
This would naturally lead to the pinnacle of Miller’s Pyramid;
“does.” If the basics have failed the referrer, and an anaesthetist
was called, we would propose the anaesthetist who attends,
not-withstanding in an emergency (when patient safety and
care is obviously paramount) acts as a facilitator, rather than
“doing it for them". The anaesthetist could critique technique,
offer tips, supervise ultrasound practice if required, and allows
a final attempt to cannulate by the referrer, before taking over
and attempting themselves. In this situation, the anaesthetist can
talk through and demonstrate any “tricks” they utilise to secure
IV access.
We would hope that if anaesthetists utilised these requests
as training opportunities, the basics would be done well
consistently, reducing primarily the number of failed attempts,
thus reducing the risks associated with multiple punctures.
Similarly, although there is an initial time investment, there
would be significant benefits to patients and the anaesthetic
workforce alike.
Patient care would be improved from more timely treatment by
decreasing the time taken to provide medication or fluids they
urgently need. Moreover, we anticipate that request numbers
would reduce, ensuring that anaesthetists are only called for
truly difficult ones, where other methods of access are genuinely
likely to be considered.
Conclusion
Anaesthetists can play a key role in improving peripheral
vascular access training for other medical practitioners. By
utilising Miller's Pyramid, we can develop a multi-step mastery
education system that will help to ensure that all healthcare
professionals have the skills and knowledge they need to
provide safe and effective vascular access.
Susan Baird
CT3 , Altnagelvin Hospital, Londonderry
Fearghal O’Brien
CT2 , Belfast City Hospital, Belfast
References
- Miller GE. The assessment of clinical skills/competence/
performance. Academic Medicine: Journal of the Association of
American Medical Colleges. 1990 Sep; 65 (9 Suppl): S63-7.
- Marc Zosky, Emilio Volz, Alex Koyfman, Stephen Alerhand.
Ultrasound Guided Peripheral Access- Tips for Success, 2016.
www.emdocs.net/ultrasoung-guided-peripheral-intravenous-linestips-for-success/ (accessed 29/09/2023)